Will a Pfo or Asd Make a Baby Sleep Alot
What is a PFO?
PFO stands for Patent Foramen Ovale. A uncomplicated way to think of PFO's is as a pigsty in the main interior walls of the heart. In the image below, y'all can see where the hole forms a connection betwixt the left and right atrium, aka the upper chambers of the heart. Information technology is a very common center status, affecting a quarter of the population .
At myheart.net we've helped millions of people through our articles and answers. At present our authors are keeping readers up to date with cutting border heart affliction information through twitter. Follow Dr Ahmed on Twitter @MustafaAhmedMD
Follow @MustafaAhmedMD
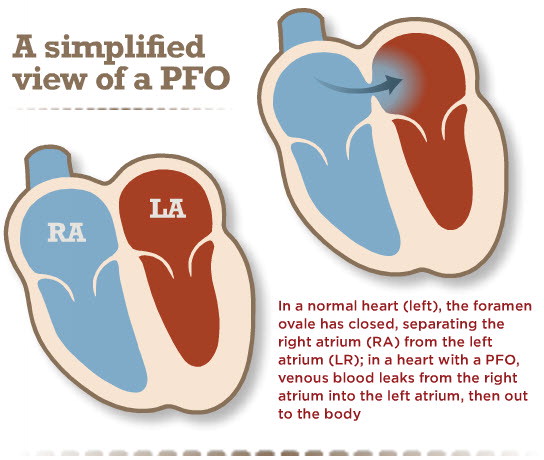
Before birth, in developing babies, this connexion is important. Why? In the womb, babies don't breath air to get oxygen in to their blood. Instead they take oxygen rich blood from their mothers. This blood is delivered to the right side of the center, simply it needs to get to the left side so information technology tin can be delivered to the trunk. It gets to the left side through the PFO. The hole is called a foramen ovale. After birth the infant begins to breath and no longer needs this pigsty. In most people this closes and seals close. In 1 in 4 people even so information technology stays open and is called a patent foramen ovale, or PFO.
How Practise We Diagnose a PFO?
PFO'due south are typically diagnosed by ultrasound scans of the heart (echocardiograms) performed as part of a work up looking for suspected eye disease. The about common initial exam when looking for a PFO is an ultrasound browse known as a transthoracic echocardiogram (TTE). As part of this test, micro-bubbles are injected into the claret through an 4. The scan is then inspected to see whether these bubbling pass from the upper right to the left side of the eye. If they exercise, it suggests communication between the chambers, such as a PFO. Oftentimes patients will be instructed to cough during the test to increase right-sided eye pressure to facilitate passage of bubbles through the PFO, this increases the chance of diagnosing a PFO. The echocardiogram is besides useful in picking upwardly structures in the eye that are thought to confer a slightly higher risk of complications in a PFO.
[wp_hyena imageurl='https://myheart.net/wp-content/uploads/2015/07/PFO-Diagnosis-Echocardiogram.gif' data_hyena='{"slate":"300,0,0″,"player_fade_speed":"500″,"on_scroll":true,"style":1}']
A more invasive way of diagnosing a PFO is a transesophageal echocardiogram (TEE), which is an ultrasound scan performed via the use of an ultrasound probe that is passed in to the food pipe where is it close to the heart. The pictures of middle structures seen in a TEE are generally much clearer than in a TTE and and then the diagnosis of a PFO can be made with greater accuracy. Because of its less-invasive nature a TTE is the initial pace in diagnosis. If closure of the PFO is planned, or if greater item of associated structured is required, then a TEE may be performed.
Is A Hole in the Heart equally Serious as it Sounds?
The vast majority of people with a PFO are healthy and will remain healthy with no issues attributed to the PFO. In fact nearly people will never need to know about information technology, and don't need to know about it. Over the years however there has been some reported associations of PFO with conditions such as stroke and migraine. I will discuss these in a footling more detail below.
Rarely the PFO can be fabricated an effect by the presence of other atmospheric condition such as critical illness, chronic lung affliction, obstructive slumber apnea, or right-sided middle failure. In these cases, the increased pressures on the right side of the centre may potentially crusade increased amounts of blood to travel through the PFO to the left side of the heart. This means non-oxygenated blood from the correct side will mix with the oxygenated blood from the left side and lead to generally lower oxygen levels, causing shortness of jiff. This is a procedure called shunting and desaturation. In some cases of significant shunting it may be recommended that the PFO exist airtight. These situations are relatively rare however.
Is There a Link to Migraines?
Some researchers have suggested a relationship between the presence of a PFO and occurrence of migraine headaches. One of the suggested reasons is that substances in the blood that are normally filtered out on the right side of the centre and the lungs, are able to get to the left side of the heart and therefore to the brain, through the PFO. In that location is no definitive proof of this all the same, and it remains a theory without scientific ground. Whether endmost the PFO makes this amend remains an ongoing debate. Some studies suggested that closure of the PFO might lead to resolution of the migraines and improvement in symptoms in a meaning proportion of people. A written report that was specifically performed to investigate the effect of PFO closure on migraines demonstrated no significant correlation between closure of the PFO and headaches. However, there are some concerns with the trial blueprint. There are 2 further ongoing trials looking at whether PFO closure tin can be effective equally a migraine handling. Hopefully these trials volition help to requite the states a clear answer. For at present, there appears to be no good bear witness to suggest PFO closure in those with migraines. Lets meet what the ongoing trials show.
Does a Hole in the Heart Crusade Strokes?
Around 800,000 people a year in the US have a stroke, and of those, almost 200,000 are repeat strokes . Up to twoscore% of these strokes do not accept a articulate cause, and these are known as cryptogenic strokes. Then what does PFO have to do with strokes? A PFO allows blood to go from the correct side of the heart to the left. In addition to blood, stroke-causing materials such as clots, gas bubbles, or other particles can travel through the PFO and potentially to the brain, causing a stroke. For this reason at that place has been much involvement in the role of PFO closure and stroke, or recurrent stroke prevention.
Over the years, several studies have suggested a higher incidence of cryptogenic stroke in patients with PFO. This would advise that in people that don't have an otherwise identifiable cause for their stroke, a PFO might exist related. The trouble is, despite the good circumstantial evidence linking PFO to cryptogenic stroke, studies designed to specifically expect at this have not demonstrated a physical clan. The big question is, in those patients who have had a cryptogenic stroke, and who have a PFO, should the PFO exist airtight. I talk about this in more detail beneath.
Possible High Take chances Features
The PFO is like a tunnel between the upper right and left chambers of the heart. Over the years, researchers have suggested a number of features of a PFO that may be associated with a college take chances of neurological events such every bit stroke. These features include, a long PFO tunnel, a very mobile floppy tunnel (known as atrial septal aneurysm), and the presence of strands that persist from fetal development (known equally Chiari strands). Although several studies have suggested that the presence of these features may confer a higher risk of stroke, these are non definitive and do not conspicuously suggest a need for closure. Further studies are needed earlier conclusions tin be reached.
Should I Accept Surgery to Close the Pigsty in My Heart? & Other Common Questions
Virtually people with a PFO will never demand anything doing about information technology, and can consider themselves to have something that is relatively common and that wont ever bother them. There are some cases where closure is recommended such as occupational hazards (come across below for deep sea defined), and in those patients where the PFO is causing oxygen levels to exist low. The more debatable indication to close a PFO is in those patients who have had a cryptogenic stroke. This is discussed in more than detail below.
Should Patients With A Stroke Have Their PFO Closed?
Even though the incidence of PFO is higher in those with cryptogenic stroke, the occurrence of stroke is still very depression in those with a PFO. Due to this fact specialists are undecided on whether PFO'southward should be closed in stroke patients. What is clear is that when someone has a stroke they should be investigated aggressively to look for underlying causes. If a cause is found then that should be treated aggressively. If appropriate investigations are performed and no cause found then it'due south by definition a cryptogenic stroke. In those with a cryptogenic stroke, the argument is that since a PFO is nowadays, that may be a cause and and then it should be airtight to preclude a potentially devastating echo stroke. The argument confronting this is that there is no guarantee at all that closing the PFO will foreclose a echo stroke, and since it is still a heart process with some underlying gamble, (admitting depression), it shouldn't exist airtight.
Until recently, closure of PFO'due south was performed very commonly, specially in patients that had a cryptogenic stroke. Older studies suggested that the recurrence of stroke was lower in stroke patients that had their PFO closed. The problem with these studies were that they were not well-designed studies that were performed to specifically address the question. Basically there were notwithstanding many unanswered questions. In recent years however, a number of relatively well-designed studies were performed to see if PFO closure, in patients that had a cryptogenic stroke, would reduce the occurrence of echo stroke.
These trials demonstrated that closure of PFO's was non proven to reduce the hazard of recurrent stroke. Those that didn't believe in closure of PFO's now had evidence to suggest that in the majority of stroke patients, the PFO should not be airtight and this had been proven in specifically designed trials. Those that strongly believed in PFO closure felt that the trials were flawed in that there were not enough patients to draw definitive conclusions given the relatively depression incidence of events. There were also issues with the fact that dissimilar devices were used in the unlike trials.
So what did we acquire for certain? ane) The incidence of recurrent stroke in patients who accept had a stroke is still relatively depression despite the presence of a PFO. 2) The main focus should be on aggressive handling for hazard factors of stroke with advisable medical therapy, earlier any consideration of a procedure for PFO closure. 3) The trials designed to look at whether a PFO should be closed in stroke patients did non demonstrate a benefit of using a device to close the PFO.
What Practice the PFO Guidelines Say?
Guidelines are non perfect, but rather they try to brand recommendations based upon the latest evidence bachelor and the highest quality of show bachelor. Given the results of the contempo trials, the guideline commission assigned a Form Iii, no benefit recommendation for device closures of PFO's. Essentially this ways they don't recommend that PFO's be closed, even in patients who have had a stroke .
This was not received well past proponents of PFO closure, every bit they felt a class IIb and not a class Iii recommendation should be applied given that uncertainties remained. A grade IIb would have essentially meant that treatment may have some benefit only the possibility of neutrality has not been excluded.
Well-nigh specialists are agreed on the fact that there is a group of patients that will benefit from PFO closure. It's just that we don't yet know who that group are. Further trials will be required to clarify these bug, but information technology's unknown whether these will ever exist performed.
What Do I Tell Patients Sent To Me For PFO Closure?
The latest guidelines accept now come up out and basically not recommended that PFO'southward exist closed routinely, fifty-fifty in the setting of stroke. Despite that, I have patients sent to me regularly for PFO closure. There are several reasons for that. Guidelines are not the police force of the land, although they are there in the best interests of patients for the mainstay. Specialists and physicians may not entirely agree which may often be reasonable, but also it is a fact that each case needs to be dealt with individually. For case I may be sent a patient by a neurologist who has a patient that has had a big debilitating stroke. Investigations demonstrated no clear crusade and no other obvious take chances factors. There is a presence of a PFO with possible high-chance features (such as features of the PFO, or a clot in the veins). The specialist feels strongly that the PFO should be closed based on these and other reasons.
The best arroyo is to have an open discussion with patients. This includes information most the procedure itself. In the right hands, the procedure can exist done safely, with minimal discomfort, and the patient sent abode the next twenty-four hours. Although complications are possible with any procedure, the rate of complications with a correctly placed device is very low. Although many patients take discussed the suitability of the procedure with their specialists who feel they volition benefit, it's of import to discuss the fact that the trials performed demonstrated that in the majority of such patients, there was no clear benefit seen from PFO closure. It's also important that prior to consideration of device closure that a thorough work up for underlying causes of stroke has been performed. I personally value the stance and involvement of a neurologist.
How Are They Closed?
Information technology is very rare present that anyone would demand surgery to close a PFO. PFO's are closed percutaneously, whereby a small tube is inserted in to a vein in the leg and passed upward to the eye. A closure device is so passed upwardly to the middle through this tube across the PFO, and and so the device is seated beyond the hole and secured in position. Ultrasound imaging is typically used to ostend device positioning. The procedure is near painless and done under moderate sedation. In experienced easily the procedure takes between thirty minutes to an hour. Equally far every bit eye procedures become PFO closure is amid the safer. As with any procedure in that location is a chance of complications. The chance of serious complication (device dislodgment, infection, damage to vessels etc.) is less than 1%.
[wp_hyena imageurl='https://myheart.internet/wp-content/uploads/2015/07/PFO-Closure-Part-three.gif' data_hyena='{"slate":"300,0.0,0″,"player_fade_speed":"500″,"on_scroll":true,"way":1}']
Diving and Decompression Sickness with PFO's
Scuba diving is popular and relatively rubber, however some divers are known to suffer from a miracle known as decompression sickness. This is where nitrogen bubbling form in the tissues during the ascension process. These bubbles can potentially cause local damage or find their fashion in to the vein blood stream. It is possible in those with a PFO the bubbles can travel through the PFO from the venous right system to the left sided arterial organization that supplies the body with claret. One time bubbles are in the arterial system they tin can potentially travel to the brain or tissues causing neurologic symptoms such as stroke or breathing difficulty. Pocket-sized amounts of bubbles in the veins are common after diving, the amounts are usually small, and cause no symptoms. Uncommonly, there may be a high chimera load that can be associated with symptoms either from the bubbles travelling to the lung, or through bubbles traveling through the PFO with associated symptoms, such as seen in decompression sickness.
So what's the current consensus regarding diving and PFO? PFO'due south are common and in full general it's non recommended that all divers be screened for this. Defined at work in detail should have advisable prior medical examination. In full general information technology would appear reasonable to screen those who have symptoms, particularly when diving, for a PFO, specially those with neurologic symptoms. Although closure of the PFO may prevent shunting of bubbles and has been reported to improve symptoms in cases, there is no strong evidence and consensus opinion on the all-time course of action in this setting. In those with significant symptoms determined to have a PFO, consultation with a cardiologist, ideally in some way familiar with diving practices should be sought, then discussion tin take identify regarding management and suitability/appropriateness of closure.
Source: https://myheart.net/articles/patent-foramen-ovale-pfo/
0 Response to "Will a Pfo or Asd Make a Baby Sleep Alot"
Post a Comment